An ongoing dialogue on HIV/AIDS, infectious diseases,
February 17th, 2026
Two Things Can Be True: The FDA Process Was Inconsistent, and the mRNA Vaccine Data Were Disappointing
Any time I write about vaccines, especially mRNA vaccines, things get dicey. Any negative comments might fuel attacks from one wing that I’m trying to fuel vaccine doubt, or (from another), hostility toward corporate innovation and profits. And of course, there’s a small but vocal minority that believes that all vaccines are inherently harmful; it’s hard (some say impossible) to reason with this group.
Still, this recent episode involving Moderna’s mRNA influenza vaccine is too important for card-carrying ID doctors like me to ignore. So here we go.
What Happened — the Meaning of “Acceptable” (and the FDA Leadership) Changed
Moderna conducted a large, global, randomized, blinded, phase 3 trial of its mRNA seasonal influenza vaccine, enrolling roughly 40,000 participants. Such studies are enormous undertakings; they represent hundreds of millions of dollars in investment and thousands of participants’ and investigators’ time and trust.
The control arm used a licensed, standard-dose influenza vaccine. According to company statements, the FDA had previously cleared this trial design.
Did they? Moderna quotes the FDA’s guidance they received before the study started:
While we agree it would be acceptable to use a licensed standard dose influenza vaccine as the comparator in your Phase 3 study, we recommend you use a vaccine preferentially recommended for use in older adults by the ACIP (i.e., Fluzone HD, Fluad or Flublok) for participants >65 years of age in the study. Data on comparative efficacy of your vaccine against an influenza vaccine preferentially recommended for use in the >65 years age group may help inform ACIP’s recommendation for the use of your vaccine in the older adult population. If you proceed with using a standard dose influenza vaccine comparator in participants ≥65 years of age, we agree with your plan to include statements in the Informed Consent Form.
That word — acceptable — is right there in the first sentence, subsequent caveats notwithstanding. The study went forward with the standard-dose vaccine.
After the trial was completed and submitted, however, on February 3 the FDA declined to review the application; here’s why:
This is because your control arm does not reflect the best-available standard of care in the United States at the time of the study. I note that this determination is consistent with FDA’s advice given to you prior to your study.
Jeepers. I guess “acceptable” wasn’t “acceptable” after all!
Regulators do sometimes reconsider positions as new data emerge — especially when a transformative study changes the standard of care.
But here, regarding the efficacy of the high-dose vaccine in older adults, the data are mixed — one study in the New England Journal of Medicine showed a benefit, another study (in the same issue) didn’t. And even though the high-dose vaccine is recommended for older adults here in the United States, this is not routine practice globally, including in some of the countries Moderna ran the study.
Should the FDA have formally reviewed the study given this sequence of events? I believe so. And if the agency had serious concerns about the adequacy of the control arm for older participants, those concerns should have been made unmistakably clear before the trial was launched.
The very fact that the head of Health and Human Services has a well-known reputation for anti-vaccine views raises concerns that this “refuse to file” action had political motivations, though no doubt the FDA would deny this. Importantly, there would be no requirement, after review, that the FDA fully approve the vaccine for use in the U.S. market. They could review it, provide formal feedback about what additional data are needed, and await a response from Moderna.
Another Disappointment — The Data
The regulatory controversy generated headlines, but disappointing in a different way are the results — not just of the Moderna mRNA flu study (October 23, 2025 presentation), but also one conducted by Pfizer for its own vaccine.
Moderna’s large trial indicated a modest but statistically significant reduction in symptomatic influenza illness relative to standard vaccination — about 27% better (2.1% vs 2.7%) — with efficacy consistent across baseline age groups. Pfizer’s phase 3 study also showed superiority over licensed influenza vaccines, with a relative vaccine efficacy of 35% against symptomatic illness; however, in subgroup analyses of older adults, the prespecified noninferiority criterion was not met. Neither program demonstrated clear differences in hospitalization or death, which are difficult to power for in seasonal influenza trials, as these events are rare.
The real problem, however, is the tolerability profile of these vaccines. They trigger more short-term symptoms than the number of influenza cases they prevent. Given the low absolute risk of influenza in these trials (<3%), symptoms of fever (6%) and chills (23%) were more common after mRNA vaccination than laboratory-confirmed influenza in either arm of the study. The company slide set characterizes these reactions as “mostly mild to moderate and of short duration” — yes, this is true, but at the same time they occurred more frequently than with the standard flu vaccine.
If the adverse events are transient, why does this matter? Seasonal influenza vaccination is not a one-time emergency intervention; it is an annual recommendation given to healthy children and adults alike. Despite this broad recommendation, enthusiasm for this vaccine among the public is already lukewarm at best. Here are this year’s data from Massachusetts:
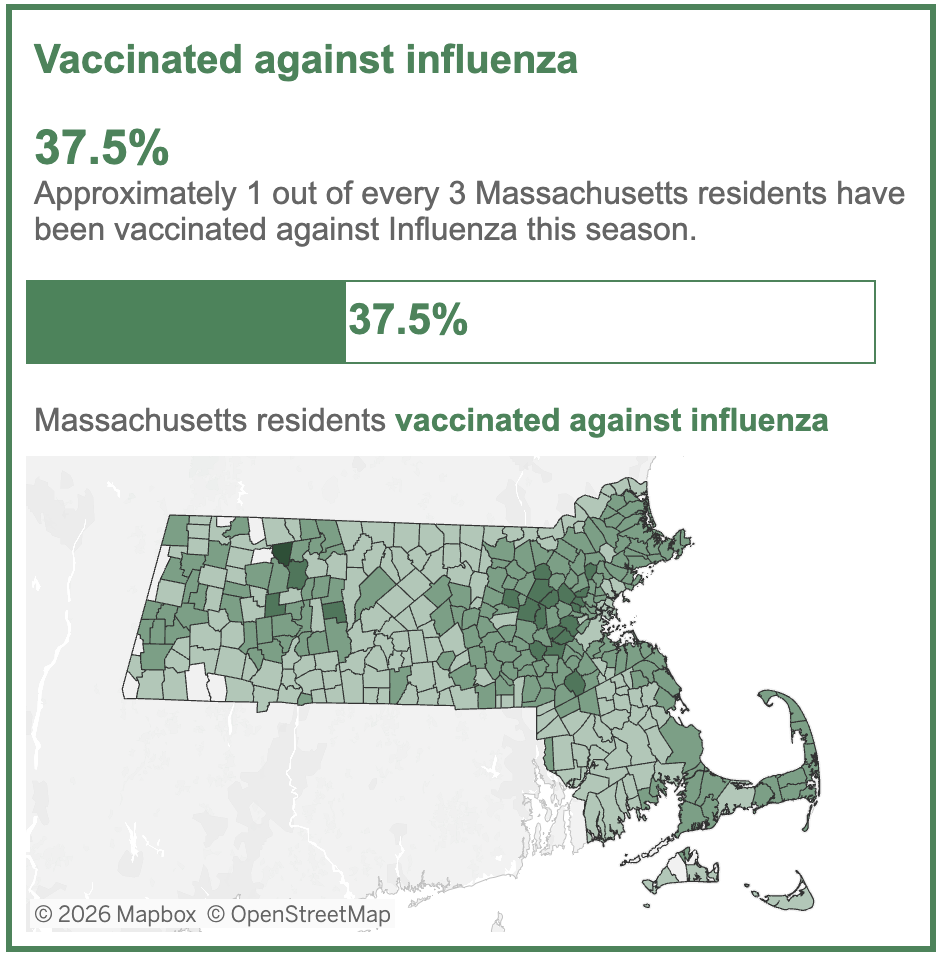
Vaccines that cause more short-term side effects without clearly superior clinical benefit will be a very hard sell in the clinic, especially on a yearly basis.
A Broader Perspective
This decision and these results are particularly disappointing given what mRNA technology demonstrated in 2020 in response to Covid-19. Traditional influenza vaccine production remains slow, dependent on strain selection months in advance and, in many cases, egg-based manufacturing. In the face of a novel pandemic strain — H5N1, H7N9, or something entirely new — the ability to design and scale a matched vaccine within weeks rather than months could be transformative.
Sometimes I’m asked what keeps me up at night in the ID universe; right up there, it’s that one of these novel flu strains becomes highly transmissible, and we’re stuck with the old way of making a flu vaccine. A formal review by the FDA of the Moderna data might have clarified a regulatory pathway for rapid approval of a strain-matched vaccine in the event of a pandemic.
One hopes that a formal review of the data ultimately occurs, with pandemic preparedness in mind.
(Addendum: The day after this posted, the FDA agreed to review Moderna’s study.)
7 Responses to “Two Things Can Be True: The FDA Process Was Inconsistent, and the mRNA Vaccine Data Were Disappointing”
Leave a Reply

Paul E. Sax, MD
Associate Editor
NEJM Clinician
Biography | Disclosures & Summaries
Learn more about HIV and ID Observations.
 FROM NEJM — Recent Infectious Disease Articles
FROM NEJM — Recent Infectious Disease Articles- Platelet-Activating Anti–Platelet Factor 4 Disorders July 30, 2026This review summarizes platelet-activating anti–platelet factor 4 disorders, including heparin-induced thrombocytopenia and related syndromes, highlighting diagnosis, antibody mechanisms, and treatment strategies.
- Case 22-2026: A 37-Year-Old Woman with Persistent Nasal Ulceration July 30, 2026A 37-year-old woman was evaluated for a 17-year history of unilateral nasal scabbing and bleeding. Nasal endoscopy showed marked, multifocal crusting and ulceration. A diagnosis was made.
- iEvac-Z, an Inactivated Ebola Vaccine — Phase 1 Study in Japan July 29, 2026Ebola virus continues to be a global threat. In a phase 1 study, an inactivated Ebola virus vaccine was tested in healthy volunteers for safety and immunogenicity.
- The Inequality–Pandemic Cycle — Rethinking Preparedness July 29, 2026Increasing pandemic frequency and increasing economic inequality are creating a self-reinforcing cycle. What’s needed is therefore a new, inequality-informed approach to pandemic preparedness.
- Phase 3 Trial of Weekly Oral Islatravir–Lenacapavir for HIV-1 Treatment July 29, 2026Among patients with HIV-1 suppression while receiving bictegravir–emtricitabine–tenofovir alafenamide (B/F/TAF), switching to weekly islatravir–lenacapavir was noninferior to continuing daily B/F/TAF in maintaining suppression.
- Platelet-Activating Anti–Platelet Factor 4 Disorders July 30, 2026
To your last point, I came across the following sadness this morning: “Staff members at the US National Institute of Allergy and Infectious Diseases (NIAID) have been told to delete the words “biodefense” and “pandemic preparedness” from the institute’s website, a move that experts say will hobble the United States’ ability to respond to future infectious disease threats, Nature reported late last week.”
The Director of the NIH recently published an article in which he stated that the current approach to pandemic preparedness is not only ineffective, but may cause pandemics (he supports the laboratory origin theory of COVID-19). He stated that the best way to prepare for a pandemic is for individuals to make better decisions about their metabolic health so that they will be less likely to become sick. Since many risk factors for bad outcomes – age, for example – are not modifiable, this seems somewhat Darwinian. In light of these views, what you have reported is not surprising.
Is there any process by which Moderna can appeal this FDA rejection? What about the Pfizer mRNA flu vaccine? Or are Prasad and RFK Jr and company going to neuter the possibility of an mRNA flu vaccine?
Pharmaceutical companies tend to want to use the weakest acceptable comparator in clinical trials. To my eyes, the memo from the FDA said they could use standard vaccine in all groups, but it would be preferable to use one of the preferentially-recommended vaccines in older patients because it would help the ACIP make recommendations later. After all, standard flu vaccines are approved by the FDA for use in elderly patients in this country. The FDA then moved the goal posts, not just by a few yards, but outside the stadium.
Despite my reservations about their choice of comparator, it is absurd that the FDA would not even review the application. But this is not about one particular vaccine. The point is to make it clear to the entire industry that anything they invest in vaccine trials could be summarily lost due to arbitrary changes in the requirements at any time. The implications are obvious and deliberate.
Thank-you, Dr. Sax, for this clarifying critique.
After plowing through the data, I too have come to the conclusion that the mRNA-based vaccine showed underwhelming efficacy, especially given its significant side effect burden. I am also concerned about the selection of the Fluarix vaccine as its comparison standard. Fluarix has demonstrated efficacy in the 65 population. However, I take Dr. Sax’s point that the FDA must show good faith when dealing with pharmaceutical companies. His conclusion, to me, at least seems reasonable; review the data from the trial and render a verdict on the vaccine. Agreeing to review it does not obligate the agency to approve it, but it does provide Moderna a pathway for designing better trials and making superior vaccines.
Governments should prioritize net health benefits—accounting for all-cause adverse events—rather than focusing solely on effectiveness. If no net benefit is demonstrated, no public funds should be allocated.