May 29th, 2012
Two-Hour ADP Can Safely and Rapidly Discharge Low-Risk Patients
Martin Than, MBBS, John Ryan, MD and James De Lemos, MD
Last year, CardioExchange’s James de Lemos interviewed Dr. Martin Than about his ASPECT study, which looked at the use of biomarkers in the Emergency Department (ED) to successfully triage low-risk patients. We welcome Than back to discuss his new JACC study, ADAPT, which examines the use of TIMI score, ECG, and troponin I alone to determine if patients presenting to the ED with chest pain could be discharged in an accelerated 2-hour diagnostic protocol (ADP).
CardioExchange’s John Ryan interviews both Than and de Lemos about how patients with chest pain can best be managed in the ED and if this approach could decrease the observation period required for these patients.
Background: In this observational study conducted at 2 urban EDs in Brisbane, Australia and Christchurch, New Zealand, blood was drawn on arrival and at 2 hours for troponin I testing using a contemporary central laboratory. Than et al found that, in patients with a TIMI score of 0 and no ECG changes, if troponin I was negative at 0 and 2 hours these patients could be safely discharged with early outpatient follow up (usually the next day). This protocol classified 20% (392 patients) of their ED population as low risk. Only one (0.25%) of these low-risk patients had a major adverse cardiac event (MACE), an NSTEMI, giving the ADP a negative predictive value of 99.7%.
Ryan: What is new with this study compared with last year’s study?
Than: There is not much difference. When we set up our cohorts in Brisbane and Christchurch we aimed to test both point of care (POC) and central laboratory testing processes. This study was run in parallel with ASPECT to answer a slightly different question. Although new POC assays are on the horizon, current commercially available contemporary central laboratory assays have better sensitivity compared with currently available POC assays. We wanted to address whether using multiple markers was necessary or if the current generation troponin I would work by itself. In reality, the diagnostic tools that we use in ADAPT are all available to us, and this made it very attractive to study.
de Lemos: Martin is too humble! In my opinion ADAPT is a really important, and practical, extension of his prior work. ASPECT was groundbreaking because it explicitly incorporated risk assessment with a rapid biomarker rule-out strategy. The limitation of that study, however, was that the biomarkers used were myoglobin (a marker that no one really knows how to use) and an insufficiently sensitive troponin assay. With this new study, they demonstrate that the principles of the prior study hold, and indeed are more powerful, using a simple rule-out strategy with troponin alone, incorporating troponin assays that are widely available in the U.S.
Ryan: How transferable are your findings to U.S. patients?
Than: I am always very cautious when asked this question, but I like to think that it would be safe. We have studied this in two countries, however, Australia and New Zealand are predominantly Caucasian without the large Afro-Caribbean population present in the U.S. Our next study will add to the evidence as we are examining the use of this algorithm in a randomized controlled trial, funded by the New Zealand-Health Research Council.
de Lemos: I think the findings are completely transferable. Low risk is low risk, regardless of patient mix. There may be a slightly lower proportion of U.S. patients identified as low risk by the algorithm (TIMI Risk Score of 0, negative ECG and troponins), particularly among African Americans, because baseline ECG abnormalities and chronically elevated troponins are more common among African Americans, due to a higher burden of hypertension, chronic kidney disease, and LVH.
Ryan: Can you put your work into context by comparing it with the recent NEJM article from Litt et al that looked at the potential use of CT angiography for safe discharge of patients with possible acute coronary syndromes (ACS)?
Than: They are reasonably complimentary. However, I do not think you want to CT angiogram everyone — there is obviously the (now small) radiation risk, the capital cost, and the challenges of the extra radiologists that you have to employ in order to have quick turnaround and reporting to make it useful. When you look at the CURE study, the group that was TIMI 0-1 had a 0.1% risk improvement (with clopidogrel) — these are the people that we are studying and that we triage with the ADP. So the NSTEMIs or UAPs that are missed would not benefit that much from NSTE-ACS therapies anyway. Then, in my mind, the intermediate group can go for a CT scan. The high-risk group should probably go straight to the cath lab, depending on your local area.
de Lemos: I think we dramatically over test the low-risk chest-pain population. Once they meet low-risk criteria as defined by the ADP algorithm or similar strategies, most of the necessary work is probably done. I’m not convinced that most of these patients need additional testing. Many of the abnormal test results have nothing to do with the presenting syndrome and represent incidental CAD in a patient presenting with non-cardiac chest pain. I would hope that the quantitative work led by Martin and his group will lead not only to shorter observation periods and fewer admissions, but also eventually to less testing. The risk is so low with a low-risk ADP that a watchful waiting strategy may be more appropriate than noninvasive testing. Of course, someone has to have the guts to actually minimize follow up testing and then report the safety of such an approach!
Than: Dead right! One of the next challenges is to subdivide the ADP low-risk patients into those requiring and not requiring onward testing. If only we had a reliable biomarker of cardiac ischaemia or plaque formation!
Ryan: What about the physicians who claim that a good history is all you need to determine if someone is having an ACS?
Than: This comes up all the time: physicians say that they can take a history and determine who is at low, intermediate, and high risk. I would challenge you to find a paper that shows that history can be used in undifferentiated patients in the ED that have normal ECG and biomarkers to predict which of the rest of the patients will turn out to have ACS with sufficient sensitivity to safely discharge the patient home. Yes, one might get it right most of the time but there are plenty of patients with atypical histories that turn out to have an ACS. I can find paper after paper that shows that historical data are not as reliably predictive as we have been taught.
Generally, the historical variables that help are age, radiation, and relationship to exertion, but, even then, they do not hold up by themselves. Risk factors only seem to be useful in young patients (age is a stronger predictor and risk factors are not independent of age). The data just do not support the claim that physicians can accurately make the distinction with sufficient safety. Being right 99 times out of 100 would make someone a pretty good diagnostician, but if they saw several hundred patients with chest pain a year the numbers of missed cases would soon build up! In the setting of an undifferentiated patient, something more than history is required to make a definitive discharge decision — that is what we offer with this study and we have the evidence to support it.
de Lemos: When I was in training I thought a good doctor could talk to a patient and determine if their chest pain was cardiac…but all these years later I am no better than I was then. I have a career’s worth of experience to tell me that there is no area in medicine that requires more humility than the chest-pain evaluation. Physicians who say otherwise, and believe they can determine if ACS is present or not by history, are fooling themselves and putting their patients at risk. This is why probabilistic algorithms, focused on risk and objective data, must guide the approach.
Ryan: Dr. Than, you say an interesting line in your paper: “In centers with lower disease prevalence, such as in the United States, it is likely that even more patients would be suitable for discharge to outpatient care with this ADP, which could potentially reduce extended observation in millions of patients annually.” Are you saying that in the EDs of the U.S., there is a lower disease prevalence? Why do you think that is?
Than: The prevalence of ACS in ED patients in the U.S. is much, much lower than in New Zealand, for example. If you look at the MIDAS study, conducted at 18 academic EDs in the U.S., there is an ACS rate of 10%, whereas it is 30% in New Zealand. I believe this is because of very good access to primary care. General Practitioners (GPs) in Australia and New Zealand handle a lot of this care and it does not reach the ED. One impact of this is that in Christchurch, for example, the admission rate into the hospital from the ED is 50%. The GPs really do a great job of seeing lower-acuity patients. In that setting, if we can get 20% of people home even with our high incidence of ACS, then in the U.S. the numbers that can be discharged might end up being even higher with use of this ADP.
de Lemos: Martin’s absolutely correct about the low prevalence in the U.S. — and the differences may be even more extreme than he suggests. In many chest-pain observation units in the U.S., the probability of ACS is less than 5%. Whether this will translate into a higher proportion of patients found to have low-risk status by the ADP is a bit of a different question, however, because many of these patients have risk factors or prior CAD, and abnormal ECGs, so while they don’t have ACS, they still may not fulfill all the criteria for early disposition from Martin’s algorithm. This sounds like a straightforward study waiting to be done.
Than: Fancy a collaboration, James?
Ryan: My uncle is in town this weekend — he is 55 years old with glucose intolerance. If he gets chest pain and has no ECG changes, am I asking the ED doctors to do a 2-hour rule out like in your study?
Than: It would be better if we did not individualize the results just yet. Institutions can look at these results and then decide as a facility or group whether they are going to change local policy over to the 2-hour ADP. So, no for this weekend, but maybe in a couple of months this option could be offered to your uncle after a good discussion between local cardiologists, internal medicine physicians, and ED clinicians.
de Lemos: I really think we’re ready to do this, provided the risk component is included, and provided the troponin assay is adequately sensitive. The only caveat would be if you brought him in very early after his chest pain started. I’d prefer in that circumstance that he hang around a few hours more.
May 29th, 2012
More Evidence Against Tight Glycemic Control
Steven Coca, DO, MS
Along with tight blood pressure control and RAAS blockade, most nephrologists recommend tight glycemic control (i.e., HbA1C < 7) for patients with type 2 diabetes, with the goals of reducing incident CKD or CKD progression. Data from observational studies has shown that tight glycemic control is associated with less albuminuria. Thus, conventional wisdom has been that tight glycemic control will improve albuminuria, and a reduction in albuminuria, in turn, should lead to less CKD. However, definitive data on the true efficacy of this strategy was lacking.
With the recent completion of the ACCORD, ADVANCE, and VADT trials, a larger body of evidence involving 28,065 patients and 163,828 patient-years of follow-up indicates that we still don’t have evidence that targeting lower HbA1C goals reduces the incidence of CKD, ESRD, or renal-related death, as published in our systematic review and meta-analysis in Archives of Internal Medicine. While the cumulative incidence of ESRD (1.5%) and renal-related death (<1%) were very low, thus underpowered to detect a difference, the outcome of doubling of serum creatinine (occurred in 4%), provided a tight confidence interval that bracketed a relative risk of 1.06 (95% CI 0.92-1.22), truly suggesting no benefit of tight glycemic control for this endpoint, even had the pooled sample size been larger. Given the fact that recent trials examining intensive glycemic control have shown no benefit for cardiovascular disease or all-cause mortality, trying to achieve tight glycemic control for the purpose of prevention of chronic kidney disease may not be worth it due to costs, patient effort, hypoglycemic risks, etc. Furthermore, even if there is a true biologic benefit for prevention of CKD, the low absolute rates of CKD events makes the achievable absolute risk reduction via intervention very small, resulting in a very high number needed to treat to prevent one CKD event. Therefore, it will take a very large randomized controlled trial with long duration of follow-up to prove that intensive glycemic control is beneficial for CKD. Until then, “less may be more”.
May 24th, 2012
Aspirin Found to Prevent Recurrent Venous Thromboembolism
Larry Husten, PHD
Aspirin can help prevent the recurrence of venous thromboembolism (VTE) after discontinuation of anticoagulation therapy, according to results of the WARFASA (the Warfarin and Aspirin) study published in the New England Journal of Medicine.
Following 6 to 18 months of oral anticoagulation, 403 patients with first-time unprovoked VTE were randomized to aspirin (100 mg daily) or placebo for 2 years. Aspirin therapy resulted in a significant reduction in VTE but did not increase the risk for bleeding:
- VTE recurrence: 6.6% per year with aspirin versus 11.2% with placebo (hazard ratio 0.58, CI 0.36 to 0.93, p=0.02).
- Major bleeding occurred in one patient in each treatment group.
In an accompanying editorial, Richard Becker writes that the results of WARFASA “are compelling and may signal an important step in the evolution of care” but calls for additional studies to more precisely define the role of aspirin in preventing recurrent VTE. The results of a larger trial, the Aspirin to Prevent Recurrent Venous Thromboembolism (ASPIRE) study, will be reported this year, according to Becker, and, in conjunction with WARFASA, “may provide more reliable evidence of the effect of aspirin in patients with first unprovoked venous thromboembolism.”
May 24th, 2012
The Next Phase in Outcomes Research: PCORI-Funded Projects
Harlan M. Krumholz, MD, SM
![]() The Patient-Centered Outcomes Research Institute (PCORI), which was established by the 2010 Affordable Care Act, announced on May 22 that it seeks to distribute $120 million in research grants. I serve on PCORI’s board of governors.
The Patient-Centered Outcomes Research Institute (PCORI), which was established by the 2010 Affordable Care Act, announced on May 22 that it seeks to distribute $120 million in research grants. I serve on PCORI’s board of governors.
The purpose of the funded projects will be to generate knowledge that enables patients and their caregivers to make better-informed healthcare decisions. Grants will focus on comparative-effectiveness studies in 4 categories:
- assessment of prevention, diagnosis, and treatment options for patients
- health system interventions
- communication and dissemination strategies
- interventions to reduce or eliminate disparities
The success of this effort will depend on the strength of each and every funded project. So we are looking to patients, researchers, clinicians, and administrators around the country to collaborate and develop outstanding proposals.
An essential ingredient is that patients and their caregivers be genuinely involved in the design, implementation, dissemination, and adoption of the research. We at PCORI believe that although patients may not be experts in research, they are experts in their own experience. That principle is fundamental to what we aim to achieve.
For more perspective on our goals and our mission, please watch a video of a brief talk about PCORI that I gave in February. Click here.
To review the funding opportunities, click here.
Then, here on CardioExchange, share your thoughts about PCORI’s approach and about the research that needs to be done.
May 23rd, 2012
FDA Advisory Committee Recommends Against ACS Indication for Rivaroxaban
Larry Husten, PHD
The FDA’s Cardiovascular and Renal Drugs Advisory Committee voted today against adding an indication for acute coronary syndromes (ACS) to the label of the anticoagulant rivaroxaban (Xarelto). The vote was 6 to 4 against approval, with 1 abstention.
The advisory panel spent most of the day trying to reconcile diametrically opposed views of the pivotal ATLAS ACS 2-TIMI 51 trial. On the one hand, the sponsor (Johnson & Johnson) and the TIMI investigators (Jessica Mega, C. Michael Gibson, and Eugene Braunwald) portrayed a robustly positive trial that strongly demonstrated the beneficial effects of low-dose rivaroxaban in ACS when added to dual antiplatelet therapy. On the other hand, one FDA reviewer, Medical Team Leader Tom Marciniak, raised multiple questions about the validity of the trial and its conclusions because of an alarming amount of early withdrawals and missing data. His view was largely endorsed by several committee members, including Steve Nissen and Sanjay Kaul.
In a press release, J&J said it “will ensure the questions raised today are addressed with the FDA.”
May 23rd, 2012
Panel: Azithromycin and Cardiovascular Risk
Paul Sax, MD, Joseph S. Ross, MD, MHS and Jeffrey Lance Anderson, MD
We asked three experts to comment on a recent study in the New England Journal of Medicine showing that the antibiotic azithromycin is associated with increased risk for cardiovascular death.
Study Results
Data from a large retrospective cohort study, in a Medicaid population, showed that azithromycin conferred a nearly threefold increase in risk for CV death and a nearly twofold increase in all-cause mortality during the 5 days of therapy, relative to no treatment.
When azithromycin and amoxicillin were compared, there were 47 excess CV deaths per 1 million courses of azithromycin. For patients with the highest CV risk at baseline, there were 245 excess deaths per 1 million azithromycin treatments, compared with amoxicillin. Azithromycin also posed greater risk for CV mortality compared with ciprofloxacin, but not compared with levofloxacin.
Expert Comments
Paul Sax, Brigham and Women’s Hospital
As an ID specialist, I have come to use azithromycin only in limited contexts: as a single-dose therapy for chlamydia or as the key drug in treating atypical mycobacterial infections. Azithromycin also retains its role, in combination with ceftriaxone, as a treatment for community-acquired pneumonia in the hospital. But the bottom line is that azithromycin is no longer that good for common respiratory infections in the clinic, given the high rate of resistance among common pathogens. These data suggesting possible cardiovascular risk from the drug make me even more likely to choose alternatives (such as amoxicillin-clavulanate or doxycyline) in patients at high cardiac risk.
Joseph Ross, Yale University School of Medicine
We have all been in a situation where a patient with symptoms suggestive of viral illness asks for antibiotics. We justify a decision to prescribe them by telling ourselves, “The patient will just go to the ED or another doctor for them anyway. Besides, the medication is safe.” This has led to many unnecessary prescriptions for azithromycin over the years because, we think, 5 days of an inappropriate antibiotic is somehow better than 10. Now we know, from studies like the one just published in the NEJM, that some of these medications are not safe. It often takes a large prospective study of this sort to illuminate small – but real – risks. Avoidable deaths should indeed be avoided. To do that, patients and physicians need to start having tough conversations about the risks from using antibiotics when they are not indicated.
Jeffrey L. Anderson, Intermountain Heart Institute
Azithromycin is frequently prescribed for patients who have extensive comorbidities, as it is well tolerated, easy to use (a 5-day course), and seemingly safe. However, large database studies, like the present one, can document rare but serious adverse reactions (witness the 47 excess CV deaths per 1 million courses of azithromycin, compared with amoxicillin, and the 245 excess deaths per 1 million courses among patients with the highest CV risk at baseline).
The efforts to control for selection bias in this study were commendable, but observational studies can never completely eliminate residual (unaccounted) bias. Also, it is not clear that azithromycin was prespecified as the primary focus of the investigation, as no confirmatory registry number (i.e., at clinicaltrials.gov) is given. In addition, at least 2 other suspect drugs (ciprofloxacin, levofloxacin) were studied, with levofloxacin also showing risk potential. Hence, was a correction in P values for multiple comparisons needed? The sudden disappearance of CV risk at days 6 to 10 is also curious, given the expected persistence of azithromycin drug levels during that time frame. Moreover, the equal increase in nonsudden and sudden CV death does not fully support the proposed mechanism of arrhythmic risk, raising the aforementioned question of unaccounted-for CV selection bias.
This high-quality report should nevertheless be taken seriously. However, it needs prospective replication in other large database studies with a broader representation of patients (e.g., the present report has an unusually high proportion of younger women) and with a clear prespecified hypothesis. Meanwhile, alternative, safer antibiotics (e.g., amoxicillin, ciprofloxacin) should be considered in clinical practice, especially in patients at increased CV risk. Finally, the prior negative results of CV prevention trials of azithromycin (as well as clarithromycin and gatifloxacin) may need to be reconsidered in light of our growing knowledge that the potentially beneficial effects of an antibiotic may be offset by drug-related adverse CV risk.
What’s your response to the new data on azithromycin and to our experts’ views?
May 22nd, 2012
Studies Probe Effect of CPAP and Sleep Apnea on Hypertension
Larry Husten, PHD
Two studies published in JAMA provide additional, but not surprising, information about the relationship between obstructive sleep apnea (OSA) and hypertension — and the role of continuous positive airway pressure (CPAP).
In the first study, Ferran Barbé and colleagues randomized 725 people with OSA but no daytime sleepiness to either CPAP or no active treatment. After a median follow-up of 4 years, there were fewer cases of systemic hypertension or cardiovascular events in the CPAP group than in the control group, but this difference did not reach statistical significance.
Incidence of hypertension or cardiovascular events:
- CPAP: 9.20 per 100 person-years (CI, 7.36-11.04)
- Control: 11.02 per 100 person-years (CI, 8.96-13.08)
The authors conclude that the study may have been underpowered to find a significant difference, though they also speculate that CPAP may be less effective in OSA patients without daytime sleepiness.
In the second study, José Marin and colleagues followed 1889 people without hypertension who had a sleep test. Over a median follow-up of 12 years, OSA was associated with an increased risk for developing hypertension, and treatment with CPAP was associated with a lower hypertension risk.
Adjusted hazard ratio for hypertension (compared with controls without OSA):
- OSA ineligible for CPAP: 1.33 (CI 1.01-1.75)
- Declined CPAP: 1.96 (CI 1.44-2.66)
- Nonadherent to CPAP: 1.78 (CI 1.23-2.58)
- CPAP therapy: 0.71 (95% CI 0.53-0.94)
The authors comment that their study is “clinically relevant considering that OSA, despite a high prevalence in Western populations, remains overwhelmingly unrecognized and untreated.” Although it was not a randomized study, the results strongly suggest “that OSA may be an independent modifiable risk factor for development of new-onset hypertension.”
In an accompanying comment, Vihesh Kapur and Edward Weaver discuss the limitations of the studies but write that the research contributes to the considerable body of evidence that “supports the role of identification and treatment of OSA to improve symptoms, quality of life, and cardiovascular end points.”
May 22nd, 2012
iFR: A New Tool to Measure Functional Ischemia
Justin E Davies, MD, PhD, Richard A. Lange, MD, MBA and L. David Hillis, MD
The instantaneous wave-free ratio (iFR) is a pressure-derived index of stenosis severity that does not require adenosine administration. The index was introduced at the 2011 TCT conference and validated by the results of the ADVISE study, published in December 2011. Following a series of presentations at the recent EuroPCR congress, Dr. Justin Davies answers questions about iFR from CardioExchange Interventional Cardiology co-moderators Richard Lange and David Hillis.
Lange & Hillis: Interventionalists are familiar with the use of fractional flow reserve (FFR) to identify hemodynamically significant coronary artery stenoses, but the concept of instantaneous wave-free ratio (iFR) is new. Can you briefly explain iFR and how the measurement is obtained?
Davies: iFR is a pressure wire-based technology for measuring the severity of a stenosis. It differs from conventional FFR in that it does not require administration of an hyperaemic agent, such as adenosine. In practice for interventionalists, the technique is identical to measuring FFR, except that when the pressure wire is advanced beyond the stenosis, the data from five beats are taken at rest, after which an assessment of iFR made.
Lange & Hillis: The validity of iFR depends on the assumption that myocardial resistance during a specific part of diastole (iFR) is similar to the resistance calculated from whole-cycle averaged measurements during maximal hyperemia (FFR). Is this true?
Davies: We know from simple physics that pressure is proportional to flow when resistance is constant (Pressure = Flow × Resistance). Previously it was not possible to stabilize resistance by administering a hyperemic agent without affecting the hyperemic state; this was the measure of achieving stable or constant resistance. Now, with advances in sensor technology and computational processing, it is possible to identify a period of stable and constant resistance during the wave-free period in the cardiac cycle. By not having to rely on an hyperemic agent to stabilize resistance, iFR may be more stenosis specific, because it is less dependent on the response of the microcirculation and myocardium to the hyperemic agents that are widely used.
Lange & Hillis: How well does iFR correlate with FFR?
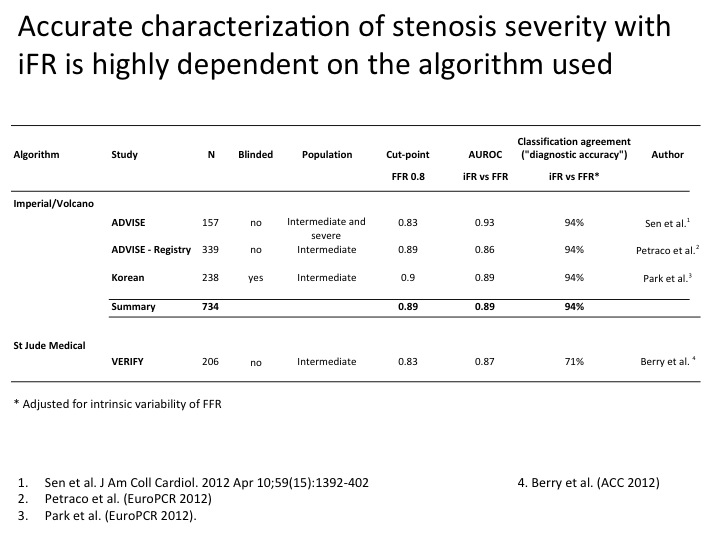
Davies: Three studies have been performed using the Imperial–Volcano iFR algorithm, and one (Verify) has been performed using the St Jude algorithm (see summary here).
{kind=link}
In the three studies using the Imperial–Volcano algorithm (734 patients from ADVISE, ADVISE-Registry, and the South Korean prospective blinded study), a strong correlation between iFR and FFR is present, the variance is low (around 5%), and the diagnostic accuracy is excellent (94% after adjustment for intrinsic variability of FFR – based on the gold standard DEFER reproducibility data).
In the study using the St Jude algorithm, the correlation was not as good, and the variance was far greater.
Lange & Hillis: An FFR <0.8 is considered abnormal (i.e., indicative of a hemodynamically significant coronary stenosis). What value for iFR is considered abnormal?
Davies: In over 700 patients (3 studies in patients with clinically intermediate stenoses), the cut-point is consistently 0.89 (for FFR, as noted, it is 0.8).
Lange & Hillis: FFR is potentially erroneous in individuals with elevated coronary venous pressure or serial coronary lesions. What is known about iFR measurements in these conditions?
Davies: iFR shares many of the physiologic features of FFR and thus is subject to many of the same limitations. Since it doesn’t require a response to adenosine, it may be less dependent on a response from the microcirculation and myocardium and, therefore, more “epicardial specific.”
Lange & Hillis: Under what conditions is iFR least reliable (atrial fibrillation)?
Davies: Our studies involve “all comers” (with the exception of individuals with severe valvular disease). We included patients with atrial fibrillation, ventricular ectopy, etc. The algorithm relies on tracking both the ECG and the pressure waveform, so it is robust; as a result, we can calculate iFR in almost all situations (99.9%). Below is a figure of a patient we saw recently who had atrial fibrillation. You can see that the iFR is very stable, despite considerable variability in the RR interval.
Otherwise, as noted, the limitations are similar to those of FFR (i.e., very small vessels [<2 mm in diameter] and distal territories where flow is very slow [these patients were not enrolled in many of FFR validation studies]).

Lange & Hillis: One of the major criticisms of iFR is that the agreement between the two methods is better for very high, nonsignificant FFR values (>0.85) than for values that indicate hemodynamically significant stenoses. In the clinically relevant range of FFR between 0.60 and 0.90, the correlation between iFR and FFR is rather poor. In what percentage of individual cases would disagreement between iFR and FFR result in reclassification of a stenosis from nonsignificant to significant — and vice versa?
Davies: This is a great question.
The original ADVISE study was an evaluation study; as such, it was designed to test the validity of iFR across a range of physiologic stenosis grades — in a manner similar to the original FFR studies. Clearly, this is not fully representative of a typical patient population. Therefore, we designed the ADVISE-Registry with a simple protocol, and we tested the reliability of iFR in a clinical population. We recruited subjects with angiographically intermediate stenoses. In total, we recruited 312 patients (with 339 stenoses), more than 80% of whom fell within the 0.6–0.9 range. Importantly, however, rather than defining this group by an arbitrary range, we assessed the population with intermediate stenoses seen by all cardiologists daily. Therefore, our results (94% diagnostic accuracy) reflect the patients who are seen every day. We were very careful not to interpret a correlation coefficient over a restricted range assessment, after the recent publication in the BMJ by Bland and Altman. This article specifically cautioned against making any assessment of correlation by reducing range, “Correlation coefficients are a property of the variables and also the population in which they are measured. If we look at a restricted population, we should not conclude that there is little or no relation between the variables because the correlation coefficient is small.”
iFR has a close correlation with FFR and hyperemic stenosis resistance (a pressure and flow-based index) in three studies (800 patients) using the Imperial–Volcano iFR algorithm. The Verify study is an outlier, and it suggests that many of the differences between these studies likely resulted from differences between the Imperial–Volcano algorithm and the St. Jude algorithm. This was perhaps best highlighted by the slides displayed in the Verify presentation, which identified the wave-free period running into the systolic upstroke of the next beat, rather than being restricted to the wave-free window. This difference should not be underestimated, since at this time resistance is highly unstable, and the proportionality of the pressure–flow relationship becomes unreliable.
May 21st, 2012
Rivaroxaban for ACS Gets Positive FDA Review, but Questions About ATLAS Trial Conduct Persist
Larry Husten, PHD
The FDA will offer generally positive – but also highly mixed – advice to the FDA’s Cardiovascular and Renal Drugs Advisory Committee when it meets on Wednesday to consider the supplemental new drug application for rivaroxaban (Xarelto, Johnson & Johnson) for use in patients with acute coronary syndrome (ACS) already taking dual antiplatelet therapy. The FDA posted the briefing documents on its website this morning.
The primary clinical review and the statistical review support approval for the new indication (the drug is already approved for venous thromboembolism prophylaxis and stroke prevention in AF). However, one reviewer, Thomas Marciniak, the Medical Team Leader, issued a blistering memorandum suggesting that the supporting data, plagued by missing and inconsistent records in the pivotal ATLAS ACS 2-TIMI 51 trial, “may not support the favorable statistical results.”
The primary clinical reviewer, Karen Hicks, recommended approval for the 2.5-mg BID dose (but not the 5-mg dose) of rivaroxaban for ACS. She noted that the lower dose reduced the combined endpoint of CV death, nonfatal MI, or nonfatal stroke in the ATLAS trial, with most of the benefit driven by a reduction in CV death, with little or no difference in MI or stroke. The higher 5-mg dose increased bleeding risk in the trial without providing additional efficacy, she concluded. She did not recommend a mortality indication for the label. Her views generally coincide with the reception of the ATLAS trial following its presentation and publication in the New England Journal of Medicine.
It should be noted that Hicks hedged her endorsement with a potentially significant caveat:
For the reasons stated above, I recommend approval. Should additional information become evident in the next two months that affect overall trial interpretability, I may choose to reconsider this recommendation.
The reasons for her statement are spelled out by Marciniak in his memorandum near the end of the FDA briefing document. Marciniak raises concerns about the high 12% rate of incomplete follow-up in ATLAS, writing: “because of the extent of missing follow-up in ATLAS we cannot have confidence in either the calculated mortality or CV endpoint benefits.” Marciniak raises a number of other issues, including, most ominously, an audit that uncovered three uncounted deaths in the trial which “may be the trip of the iceberg regarding problems with missing data.”
Marciniak has been down this path before, with mixed results. During the marathon 2-day Avandia meeting, Marciniak thoroughly discredited the RECORD trial, and this played a role in the generally unfavorable committee recommendations. By contrast, although Marciniak and others were highly critical of the pivotal PLATO trial during the ticagrelor (Brilinta) advisory committee meeting, the committee and the FDA ultimately approved ticagrelor. Finally, we should remember that the FDA reviewers initially recommended against approval of rivaroxaban for the AF indication due to concerns about the ROCKET trial but that the committee ultimately recommended approval, based on their support of large, pragmatic trials. Compared with the drama of that hearing, Wednesday’s session is likely to be much less contentious.
May 21st, 2012
Selections from Richard Lehman’s Literature Review: Week of May 21st
Richard Lehman, BM, BCh, MRCGP
CardioExchange is pleased to reprint selections from Dr. Richard Lehman’s weekly journal review blog at BMJ.com. Selected summaries are relevant to our audience, but we encourage members to engage with the entire blog.
NEJM 17 May 2012 Vol 366
Warfarin vs. Aspirin for Stroke Prevention in HF (pg. 1859): Here’s a big international study to settle the question of whether warfarin or aspirin is better at preventing stroke and mortality in heart failure with sinus rhythm. Well, that’s what the title would have you believe. In fact this is a truly old-fashioned study which defines “heart failure” by an ejection fraction under 35 and so ends up with a cohort of patients of mean age 61 and 80% male. It tells you nothing at all about your average patients with clinical heart failure who have a mean age of 76 and are 50+% female, half with normal ejection fractions. Their chances of going into atrial fibrillation and throwing off clots are much higher than those of this cohort. Someone needs to do a trial comparing a fixed-dose new generation anticoagulant with aspirin in this “real world” population.
CVD Risks of Azithro (pg. 1881): This study about the increased risk of cardiovascular death while taking azithromycin has got a lot of publicity. The increase in CV death for the average adult population is put 47 per million taking a five day course of this antibiotic rather than amoxicillin: it is considerably higher in those at increased CV risk, of course. But there is an easy way to remember not to give this or any other macrolide antibiotic to those at highest risk: just heed your computer warning that all these drugs interact with statins.
Another cup of Joe (pg. 1891): The paper that got the most publicity in this week’s New England Journal though was this one showing that coffee consumption is associated with lower all-cause mortality. This seems dose-related too, which is good news as I sit here all a-buzz from a mug brewed to the strength my wife likes. Legend has it that coffee reached the West via the Turkish armies who were defeated at the walls of Vienna in 1683, complete with bread rolls in the shape of the Islamic crescent. Which is still the best – and now perhaps the healthiest – breakfast; and the surest mark of advanced civilization.
Lancet 19 May 2012 Vol 379
After flirting briefly with items in the On-line First sections of the journals, I’ve largely gone back to the weekly printed items, for the sake of simplicity. But two papers on The Lancet’s website this week cry out for comment, as they put the final nails in the “treat-to-target” lipid management coffin. I hope.
Statins Work: The first one is old news, but repackaged as a huge meta-analysis of individual patient data from 27 randomized trials of statins which included subjects at low risk of cardiovascular events. Guess what? Everybody’s risk came down, whatever it was to start with. And the mortality benefit of the statin therapy was directly in proportion to the fall in LDL-cholesterol, and it far outweighed any measurable harms. So should everybody take a statin, so as to reduce the population rate of CV disease? No, I object to this kind of public-health-speak: everyone who wants to should be able to: it’s a personal choice. And does this prove that statins work by LDL-C lowering? Again no. They just work, and people should take them or not, as they wish to adjust their life chances.
We Don’t Know How HDL-C Works: And now onto the question of “good” cholesterol – HDL-C. There is a linear relationship between this lipid fraction and a decrease in cardiovascular risk. So far, 200 or more trials have been done with HDL-C raising agents; and not one of them has succeeded. Roche has just terminated its trial of dalcetrapib for futility, leaving the Oxford CTSU trial of anacetrapib (REVEAL) about the only one left standing. I wonder if it will ever recruit its 30,000 subjects. Here a massive Mendelian randomization study shows that the HDL-C/CV protection association is unlikely to be causal, and plasma measurements of HDL-C may actually tell us very little.
BMJ 19 May 2012 Vol 344
AAA: A study from the Highlands and islands of Scotland looks at mortality in men screened for abdominal aortic aneurysm. I was somewhat fazed to see this defined by an aortic diameter of 30mm or more: in the MASS study and in my clinical practice, the threshold was 55mm. But this is only a fairly crude associational study which unsurprisingly shows that the diameter of the aorta in old men is a marker for high cardiovascular risk and cancer risk, almost all of it attributable to smoking.
Arch Intern Med 16 May 2012
Omega-3s (pg. 686): I am an avid eater of all kinds of fish, and I think my absolute favourite is a large fresh herring fried in butter. Unfortunately you probably have to live on the West Coast of Scotland to obtain such an article: away from fishing ports you are safest with kippers, as there is nothing worse than a stale herring. Eating is meant for sustenance and pleasure. It has also been found that eating a diet rich in fatty fish is associated with better cardiovascular health – and if there is any evidence against butter, I have yet to read it. Unfortunately a large proportion of mankind seems to be averse to eating the oilier species of fish, and instead, many seek to obtain CV benefits from omega-3 fatty acid supplements. But as this systematic review reveals, there is no evidence worth the name that these achieve anything for secondary prevention following cardiovascular events.
Fenofibrate (pg. 724): Finally, an insight into the bizarre world of American lipid prescribing: target-driven, irrational, and profoundly distorted by big pharma. Fenofibrate is a drug which has repeatedly been found to have no beneficial effects whatsoever, though it lowers “bad” lipids, including triglycerides. As evidence for its uselessness mounted, fenofibrate prescribing in the USA soared, driven by advertising from Abbott Laboratories. But this $1bn-a-year triumph of marketing over evidence was due to come to an end when Abbott’s patent expired. This paper describes how Abbott fought off the threat of generic competition and continues to sell modified fenofibrate products with rights to exclusivity. Its lead author is Nick Downing, a medical student with a unique accent forged in London and Harvard, whom I met when he first began work on this at the end of his first year as a medical student at Yale last year. Well done Nick! But hang on – what is this I see on the NEJM website? A full special report on regulatory agencies in the US, Europe and Canada, with first author Nicholas Downing. For a second- year medical student to publish one paper in a leading medical journal might be called good fortune; to publish two begins to look like brilliance.
And do read this inspiring advice to Be Brave, from Nick’s mentor Harlan Krumholz.
 NEJM — Recent Cardiology Articles
NEJM — Recent Cardiology Articles- Platelet-Activating Anti–Platelet Factor 4 Disorders July 30, 2026This review summarizes platelet-activating anti–platelet factor 4 disorders, including heparin-induced thrombocytopenia and related syndromes, highlighting diagnosis, antibody mechanisms, and treatment strategies.
- Pulsatile Liver in Severe Tricuspid Regurgitation July 30, 2026A 51-year-old woman with right heart failure presented with worsening abdominal distention and leg swelling. Examination was notable for ascites, leg edema, a grade 4/6 holosystolic murmur, and a pulsatile liver (shown in a video).
- Mavacamten in Adolescents with Obstructive Hypertrophic Cardiomyopathy July 23, 2026In this trial, among adolescents with obstructive hypertrophic cardiomyopathy, the cardiac myosin inhibitor mavacamten led to a significantly greater reduction in left ventricular outflow tract obstruction than placebo.
- Cardiotoxic Effects and Microdystrophin Expression after Gene Therapy for DMD July 22, 2026In a patient with Duchenne muscular dystrophy, cardiotoxic effects developed after treatment with delandistrogene moxeparvovec. Microdystrophin levels in the heart and skeletal muscle were less than 1% of normal dystrophin levels.
- Descending Thoracic Aortic Aneurysm July 16, 2026A man presented with a 2-month history of chest heaviness and a 2-week history of shortness of breath. Pulsations were visible between his ribs (shown in a video). Ultrasonography revealed a rounded structure near the heart.
- Platelet-Activating Anti–Platelet Factor 4 Disorders July 30, 2026