February 15th, 2012
Part 1: Clashing Views of Appropriate Use Criteria for PCI
Paul S. Chan, MD, MS, J Aaron Grantham, MD, FACC, Steve Marso, MD and John Spertus, MD, MPH
In a recent Viewpoint in JACC: Cardiovascular Interventions, Marso and colleagues expressed grave reservations about the application of appropriate use criteria for PCI in a controversial study published last year in JAMA by Chan and colleagues, which found that only half of PCIs performed for nonacute indications were classified as appropriate. Interventional cardiology editors Rick Lange and David Hillis asked CardioExchange members for their opinions on this topic. In this post, Lange and Hillis initiate a series of questions to the main protagonists in the debate, Steven Marso and Aaron Grantham, on the one side, and Paul Chan and John Spertus on the other side. All the authors are affiliated with the Saint Luke’s Mid America Heart Institute in Kansas City, Missouri.
Lange & Hillis: Concerns regarding the appropriateness use criteria (AUC) for coronary revascularization (published in 2009) recently have been raised. Just last month, the 2012 update to the AUC for coronary revascularization was released. Does the update adequately address these concerns? Should the AUC be updated more often?
Chan & Spertus: The AUC represent an important, proactive approach of the profession to provide a foundation for assessing the decision-making process in choosing revascularization therapy for CAD. The original version was the first attempt to quantify the quality of decision-making and will need to be updated over time for 2 reasons: a) there are methodological limitations in accurately mapping clinical scenarios; and b) there are new data to inform judgments about the appropriateness of selecting revascularization. The 2012 updates addressed some of these issues. For instance, the 2012 AUC further refine the classification of ACS (unstable angina and NSTEMI) patients into high and low risk, incorporate new clinical trial data, such as SYNTAX, into the AUC, and provide ratings for some new indications.
Marso & Grantham: We were pleased to see the coronary revascularization AUC were updated, and recently published online. The update incorporated a handful of new indications in response to recently completed clinical studies and provide an initial approach to incorporate FFR into the appropriate use criteria. These updates also re-emphasize that an “uncertain” category as not being inappropriate. These refreshed criteria serve as a reassuring signal that the committee members are receptive to evolving these criteria over time based upon new clinical trial data. These criteria really should be malleable over time, making the coronary revascularization AUC a living document.
However, these criteria were neither intended to be nor are responsive to the systematic limitations articulated in our recent Viewpoint article. There are a number action items we proposed which were not addressed that might improve the AUC including the following broad topics:
- Reliably determining and then documenting risk based upon noninvasive imaging studies.
- Developing a strategy to seek active participation by a larger number of interventional cardiologists than are currently on the AUC Technical Panel.
- Reconsidering indication 12B, as there remains broad disagreement that this is an inappropriate category for PCI.
- Reconsidering the lumping of Class 2 with Class 1 angina for the mappable clinical scenarios.
- Considering a strategy to co-localize a stress defect with the target lesion treated.
- Developing a more comprehensive strategy to incorporate a role for FFR into PCI decision making.
Note: Part 2 of this 5 part series will be published tomorrow.
February 15th, 2012
Mortality-Risk Calculators for AMI and Heart Failure Patients
Harlan M. Krumholz, MD, SM
Two mortality-risk calculators – one for patients with acute MI and another for those with heart failure – are now available for free at www.mortalityscore.org. The calculators are based on risk models produced by our research group at Yale for the Center for Medicare and Medicaid Services (CMS). The models are derived from Medicare administrative-claims data for AMI and heart failure that the CMS reports publicly on its Hospital Compare website.
Because the models were designed to predict 30-day mortality as strongly as possible, they have more variables than we might have used in a leaner model designed for rapid clinical use. Nevertheless, the calculator can be populated with information that is easily available on admission. In about 2 minutes, you can enter data on a patient and get an estimate for his or her 30-day mortality risk.
The Center for Outcomes Research and Evaluation at Yale-New Haven Hospital has made the calculators available for free to all comers. There are no advertisements. All of the underlying data have been published in peer-reviewed articles that describe the development and validation of the publicly reported measures (see references below). We have put all of the information in the public domain.
Let us know if you find the calculators useful. And also take a look at our previous calculator on readmission risk.
References:
February 14th, 2012
Meta-Analysis: Air Pollutants Raise Short-Term Risk for MI
Larry Husten, PHD
Air pollution significantly raises the short-term, 7-day risk for MI, according to a new meta-analysis published in JAMA. Hazrije Mustafic and colleagues analyzed data from 34 studies and found a significant increase in the relative risk (RR) for MI with all the main air pollutants except ozone:
- carbon monoxide: RR 1.048, CI 1.026-1.070
- nitrogen dioxide: 1.011, 1.006-1.016
- sulfur dioxide: 1.010, 1.003- 1.017
- particulate matter ≤10 µm : 1.006, 1.002-1.009
- particulate matter ≤2.5 µm: 1.025, 1.015-1.036
- ozone: 1.003, 0.997-1.010
The authors acknowledge that the magnitude of increased risk was small, but calculated that because of the broad exposure of the population to air pollution, the attributable fraction ranged from 0.6% to 4.5% for the different pollutants.
February 13th, 2012
Heart and Stroke Foundation’s “Make Death Wait” Campaign: Advocacy or Scare Tactics?
Marilyn Mann, J.D.
Editor’s Note: This post is reprinted with permission from Marilyn Mann’s Blog.
I am interested to know what readers think of the two Heart and Stroke Foundation of Canada (HSF) ads shown below. The ads are part of HSF’s “Make Death Wait” awareness and fundraising campaign that’s been underway for the past few months.
In the first ad, shown in this YouTube video, several different women are shown on screen as a male voice, meant to personify death, intones “I love women. I love older women, professional women, stay-at-home moms. I love how women put their family first. I love how you’re so concerned that I’ll get to your husband.”
In the final scene, a woman in a bathing suit looks apprehensively over her shoulder as the voice warns, “You have no idea that I’m coming after you.” Eileen Melnick McCarthy, director of communications for the foundation, told a reporter that the intent of the campaign is to “wake up Canadians to the threat of heart disease and stroke.”
In addition, the print ad below has appeared in a Canadian magazine. The copy, in case you can’t make it out, reads as follows:
Death loves menopause. He loves that menopause makes women more vulnerable to heart disease and stroke. And that women are far more likely to die of a heart attack. Most of all, he loves that heart disease and stroke is the #1 killer of women. Please donate, and make death wait.
Is this a legitimate way to “wake up” people to the threat of cardiovascular disease? Or unnecessary and counterproductive scare tactics? I lean toward the latter.
Video: Death Loves Women. Make Death Wait.

February 13th, 2012
Selections from Richard Lehman’s Weekly Review: Week of February 13th
Richard Lehman, BM, BCh, MRCGP
 CardioExchange is pleased to reprint selections from Dr. Richard Lehman’s weekly journal review blog at BMJ.com. Selected summaries are relevant to our audience, but we encourage members to engage with the entire blog.
CardioExchange is pleased to reprint selections from Dr. Richard Lehman’s weekly journal review blog at BMJ.com. Selected summaries are relevant to our audience, but we encourage members to engage with the entire blog.
Week of February 13th.
JAMA 8 Feb 2012 Vol 307
Shared Decision Making
565 There are signs that JAMA is gradually improving under its new editor, although moving its perspective pieces to the beginning of the journal doesn’t really count as progress. The BMJ has also tinkered with its order of contents, almost as if to hide the fact that they are improving at the same time. And it will certainly take a lot more than swapping chairs around to improve The Lancet. Anyway, here is a Viewpoint piece that is well worth reading if you are interested in screening and shared decision-making with patients. In a clear and well-structured piece, the authors trace the gradual path of disillusionment from the “spotting cancer early is always good” mindset to “there are harms and costs” attitudes of the present. They point out that dumping these issues on to individual clinicians to share with patients is a dubious strategy (not least in health systems where patients are called for screening independently of their normal health care provision). “Expert groups may dispute the ‘facts’; the science can be difficult for physicians to communicate and for patients to understand; some patients demure [sic] and want the physician to decide; physicians may lack the time, reimbursement, or motivation to engage in long discussions; and social attitudes and medicolegal pressures may influence the decision.” I particularly like their concluding sentences: “However, society’s first concern should be to confirm that screening is a net good for public health. This requires harms to be considered independently of costs. Until the reality of harms becomes more palpable to clinicians and the public, concerns about the safety of screened populations will continue to be mistaken for frugality.”
567 The next Viewpoint piece also raises an important issue in shared decision-making with patients. When we mention the potential harms of the treatment we propose – as we often must – can this interfere with its effectiveness? Again I would recommend everyone to read this article on Nocebo Effects, Patient-Clinician Communication, and Therapeutic Outcomes. This is not as coherent a piece as the previous one, but it’s good to see this discussion coming out into the open. So much simplistic talk about shared decision-making ignores the extraordinary power of clinicians to instill fear and hope in their patients by the words they use and the attitudes they convey. We need to be realistic and indeed scientific about this. We have a duty to be honest, but we also have a professional and ethical duty to understand the effect we have on people in situations where they are vulnerable and we have the power to help them or harm them.
BMJ 11 Sep 2012 Vol 344
Drug-Induced Gout
In my recent experience of general practice (increasingly geriatric on both sides), about half of gout is brought on by diuretics. So it’s no surprise that this trawl through the UK GP Research Database to find associations between blood pressure lowering drugs and gout points the finger most clearly at thiazides. What is slightly less expected is that beta-blockers increase the risk of gout by around a half and ACE inhibitors blockers and angiotensin II blockers increase it by about a quarter. Except for losartan, which decreases gout risk by about 20%, as do calcium channel blockers.
February 13th, 2012
Meta-Analysis Raises More Questions About Routine Use of Aspirin for Primary Prevention
Larry Husten, PHD
Although aspirin can reduce the risk for cardiovascular (CV) events, the associated increase in bleeding suggests that it should not be used routinely in people without prior CV disease, say the authors of a meta-analysis published in the Archives of Internal Medicine.
Sreenivasa Rao Kondapally Seshasai and colleagues combined data from nine clinical studies including more than 100,000 participants who were followed for a mean of 6 years. They found a significant reduction in CV events, but not CV mortality, and an increased risk for important bleeding events:
- CV Events: OR 0.90, CI 0.85-0.96, number needed to treat (NNT): 120
- Nonfatal MI: OR 0.80, CI 0.67-0.96, NNT: 162
- CV Death: OR 0.99, CI 0.85-1.15
- Nontrivial bleeding events: OR 1.31, CI, 1.14-1.50, number needed to harm, 73
The authors conclude that in the absence of further studies identifying patients likely to benefit from aspirin therapy, “a reappraisal of current guidelines appears to be warranted, particularly in countries where a large number of otherwise healthy adults are prescribed aspirin, since a significant proportion of them may develop bleeding complications.”
In an accompanying comment, Samia Mora agrees with the authors that routine use of aspirin for primary prevention should not be recommended. But, she writes, “it is reasonable to consider using aspirin for primary prevention in higher-risk individuals without known CVD (above 1% CVD event rate per year) if they are deemed to have a greater benefit to risk ratio and after taking into account patient preferences.”
February 13th, 2012
Pop Quiz
Shengshou Hu, M.D.
To celebrate Heart Month, CardioExchange welcomes this fun bit of trivia from Dr. Westby Fisher, an electrophysiologist practicing at NorthShore University HealthSystem in Evanston, Illinois, and a Clinical Associate Professor of Medicine at University of Chicago’s Pritzker School of Medicine. This piece originally appeared on his blog, Dr. Wes.
What does this graph represent?
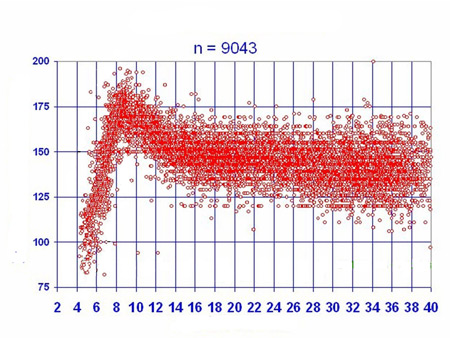
Hint: you were probably on it.
Scroll down for the answer.
The x axis is weeks (of gestation), the y axis is heart rate. The rest of the answer can be found here.
{kind=link}
I thought this was interesting because of the remarkably linear relationship of the heart rate to gestational age in the first trimester of pregnancy.
Happy Heart Month!
February 9th, 2012
The Y Chromosome May Explain Why Men Have Earlier Coronary Disease
Larry Husten, PHD
The earlier onset of coronary artery disease in men has long provoked speculation and research. Now a new study in the Lancet suggests that common variations in the Y chromosome (which is transmitted directly from father to son and does not undergo recombination) may play an important role in the increased risk seen in men.
Using genetic information on the Y chromosome, an international team of researchers identified nine different ancient lineages — haplogroups — in 3233 British men. Two of the haplogroups accounted for nearly 90% of the Y chromosome variants in subjects, and carriers of one of these haplogroups — haplogroup I — had a 50% increase in the risk of coronary artery disease compared to men with other haplotypes. This increase in risk was independent of other known risk factors. The investigators noted that haplogroup I appeared to exert a powerful effect on genes relating to inflammation and immunity. They further noted that haplotype I is generally more prevalent in northern than in southern Europe, and that this distribution is paralleled by an increased risk of coronary artery disease in northern Europe.
In an accompanying comment, Virginia Miller writes that the results of the study are “exciting because they identify a genetic haplotype linking response to infection (adaptive immunity) rather than innate immunity with perhaps an exaggerated inflammatory response and cardiovascular disease in men.”
February 9th, 2012
What Are You Doing About Readmission Rates?
Harlan M. Krumholz, MD, SM
The need to focus on readmission is becoming more relevant every day. Today there was news in the Wall Street Journal that UnitedHealth may start incorporating incentives about readmission into its contracts:
‘UnitedHealth, like other insurers, is targeting the traditional system that pays hospitals and doctors for each service provided, rewarding them for more care but not necessarily better care. Under the new plan the carrier is rolling out, part of medical providers’ compensation could be tied to goals such as avoiding hospital readmissions and ensuring patients get recommended screenings.
Unfortunately there are no easy solutions. The H2H Quality Initiative, sponsored by the ACC, is an attempt to bring together practitioners and institutions to share information about what works. [Disclosure: I co-lead this effort – but it is currently free and an effort to foster a learning community.] Take a look if you are not familiar with it: http://www.h2hquality.org/
What are you doing about the readmission rates at your institution? Have you seen any effective interventions? Has the topic been raised?
February 8th, 2012
Prominent Interventionalists Attack Appropriate Use Criteria for PCI
Larry Husten, PHD
A group of leading interventional cardiologists has launched an attack on the growing role of appropriate use criteria (AUC) for PCI in the U.S. They argue that severe flaws in current guidelines render unreliable attempts to assess the rate of appropriate procedures.
In a paper published in JACC: Cardiovascular Interventions, Steven Marso and colleagues (Paul Teirstein, Dean Kereiakes, Jeffrey Moses, John Lasala, and J Aaron Grantham) criticize a study in JAMA published last year from the National Cardiovascular Data Registry (NCDR) that found a large degree of inappropriate or uncertain PCI procedures, as well as a wide range of variability among institutions. Marso et al. write that the JAMA paper sensationalized the data by focusing attention on the low rate of appropriate indications for nonacute PCI — 50.4% — while failing to point out that the study found that 84.6% of procedures in the entire study population — acute and nonacute alike — were deemed appropriate. Furthermore, given the imprecision built into the system, they ask: What is the “acceptable threshold” of inappropriate PCI?
The authors write that the AUC panel “purposefully limited involvement of the interventional community during the development process” in order to avoid having a majority of committee members “whose livelihood is tied to the technology under study.” But the under-representation of interventionalists may have biased the results, they argue. One particular case as graded by the AUC panel was the most common reason for cases to be categorized as inappropriate: the AUC committee decided that PCI was inappropriate for a patient with 1- to 2-vessel disease, no proximal LAD involvement or prior CABG, class I or II symptoms, low-risk noninvasive findings, and on no or minimal medications. But most clinicians believe this is an uncertain but not inappropriate indication, they say. The AUC panel may have “got this one wrong,” they write.
Marso et al. also point to the “lack of specific criteria for interpreting” stress tests in the NCDR database. In addition, they disagree with the inappropriate classification of most cases of class II angina before medical therapy has been attempted, arguing that both COURAGE and BARI 2D showed that PCI is a valid option for these patients. Finally, the authors argue that the NCDR database contains numerous inaccuracies, including misclassification of patients’ angina status or noninvasive risk assessment.
One striking feature of the controversy is that two of the authors of the JAMA paper (Paul Chan and John Spertus) and two of the authors of the JACC: Cardiovascular Interventions paper (Steven Marso and Aaron Grantham) are all at the same institution: Saint Luke’s Mid America Heart Institute in Kansas City, Missouri. Marso et al. state that 56% of cases classified as inappropriate at their institution “were misclassified due to incorrectly coding CCS class status, not documenting angina equivalents, or inaccurate documentation of the noninvasive risk assessment findings.”
Until the NCDR database is fixed, Marso et al. write, “it could be argued” that the authors “should refrain from approving AUC-related clinical studies until such time that assurances are both valid and reliably collected.”
Comments on this item are closed. To keep the conversation in one place, please comment here: (In)Appropriate PCI: An (In)Appropriate Critique?
 NEJM — Recent Cardiology Articles
NEJM — Recent Cardiology Articles- Platelet-Activating Anti–Platelet Factor 4 Disorders July 30, 2026This review summarizes platelet-activating anti–platelet factor 4 disorders, including heparin-induced thrombocytopenia and related syndromes, highlighting diagnosis, antibody mechanisms, and treatment strategies.
- Pulsatile Liver in Severe Tricuspid Regurgitation July 30, 2026A 51-year-old woman with right heart failure presented with worsening abdominal distention and leg swelling. Examination was notable for ascites, leg edema, a grade 4/6 holosystolic murmur, and a pulsatile liver (shown in a video).
- Mavacamten in Adolescents with Obstructive Hypertrophic Cardiomyopathy July 23, 2026In this trial, among adolescents with obstructive hypertrophic cardiomyopathy, the cardiac myosin inhibitor mavacamten led to a significantly greater reduction in left ventricular outflow tract obstruction than placebo.
- Cardiotoxic Effects and Microdystrophin Expression after Gene Therapy for DMD July 22, 2026In a patient with Duchenne muscular dystrophy, cardiotoxic effects developed after treatment with delandistrogene moxeparvovec. Microdystrophin levels in the heart and skeletal muscle were less than 1% of normal dystrophin levels.
- Descending Thoracic Aortic Aneurysm July 16, 2026A man presented with a 2-month history of chest heaviness and a 2-week history of shortness of breath. Pulsations were visible between his ribs (shown in a video). Ultrasonography revealed a rounded structure near the heart.
- Platelet-Activating Anti–Platelet Factor 4 Disorders July 30, 2026